6. Organ Containers
6.1. Kidney
In the kidney container there are three sections:
Underlying disease (leading to transplantation)
Biopsy & Rejection and
Allograft morbidities.
6.1.1. Underlying disease
In this section we select and confirm the condition leading to transplantation.
To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other category. For example ‘Diabetes mellitus type 1’ can be entered or as ‘Condition Leading to Tpx’ or as ‘Metabolic’. It will appear in both sections, regardless of where it has been entered.
As conditions or diseases leading to transplantation in kidney we select from the following:

However ‘Diabetic nephropathy’ can not be chosen. You have to enter the underlying disease to the diabetic nephropathy as ‘Diabetes mellitus type 1’, ‘Treated diabetes mellitus type 2’, ‘Postpancreatectomy diabetes’ or ‘Post-transplant diabetes mellitus (PTDM)’.
All entered diagnosis will appear in the section ‘Underlying Disease’ and you must confirm the condition leading to transplantation.

In all causes except ‘previous allograft failure’, you can enter a possible biopsy confirming the diagnosis. Be careful to enter the Biopsy ID that confirmed the disease and not just a biopsy of the native organ.
In case of two or more conditions leading to the same transplantation, the biopsies showing the diseases could be different one from another (e.g. one showing the diabetic nephropathy and a later one showing the hypertensive nephrosclerosis). Use the first biopsy that confirmed the disease.

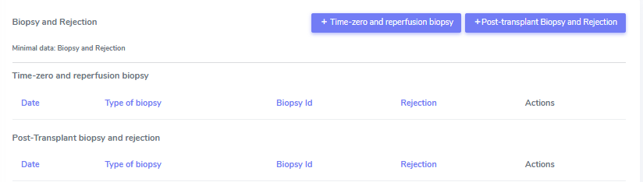
6.1.2. Biopsy & Rejection
In this section we enter biopsies and rejections. We distinguish between ‘Time zero and reperfuion biopsies’ and ‘Post-transplant biopsies’.
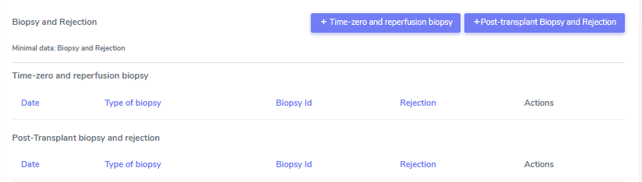
Time zero and reperfusion biopsy
In the case of a time zero or reperfusion biopsy we enter the:
Date of the biopsy
Biopsy ID
Type of biopsy
Pre-implantation (allograft)
At reperfusion
Native organ
Banff score. In the Banff score we select the values indicated in the biopsy. In case a value is not done or not listed, please choose ‘missing’. If the value can not be evaluated, select this from the drop-down menu.
If the biopsy lists one of the following diagnosis, please enter them in the ‘Allograft morbidities‘ section as ‘allograft disease’:
Acue tubular necrosis (ATN)
Chronic lesions, not specified
CNI nephrotoxicity
De novo glomerulonephritis/Vasculitis
Diabetic nephropathy
Graft pyelonephritis
Hemolytic uremic syndrome/ Thrombotic microangiopathy
PyVAN
Recurrence of initial disease or
Other (specifyng a major disease of the allograft in the comment section).
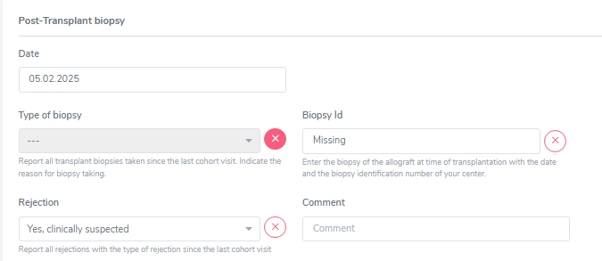
Post-Transplant biopsy and rejection
In the case of a biopsy performed after transplantation, we enter:
Date of the biopsy
Biopsy ID
Type of biopsy:
Diagnostic biopsy
Protocol biopsy or
other
Banff score. In the Banff score we select the values indicated in the biopsy. In case a value is not done or not listed, please choose ‘missing’. If the value can not be evaluated, select this from the drop-down menu. You also have the option to choose ‘All missing’ if Banff score was not evaluated in the biopsy.
In the ‘Clinical and pathological diagnosis’ part, we enter:
Rejection (Yes, biopsy proven; Yes, clinically suspected; No)
If the patient showed the presence or absence of clinical symptoms (clinical/subclinical)
The Pathology report summary/diagnosis (copy and paste this part from the biopsy report in whatever language the text is) and
If necessary, a comment.
When you select a ‘Yes’-option in the rejection field, you can choose the regimen(s) to treat this rejection in the section that appears below.
Select all that apply from the following list and do not forget to enter the treatment in the ‘Treatment’ section as drug prescription or non-pharmacological treatment:
No treatment of rejection
ATG
ATGAM
Campath
IG iv
Metyl-prednisone iv
OKT3
Photopheresis
Plasmapheresis/PE
Prednisone po
Rituximab
Thymoglobulin
Other (Specifying the treatment in the comment field)
If the biopsy lists one of the following diagnosis, please enter them in the ‘Allograft morbidities‘ section as ‘allograft disease’:
Acue tubular necrosis (ATN)
Chronic lesions, not specified
CNI nephrotoxicity
De novo glomerulonephritis/Vasculitis
Diabetic nephropathy
Graft pyelonephritis
Hemolytic uremic syndrome/ Thrombotic microangiopathy
PyVAN
Recurrence of initial disease or
Other (specifyng a major disease of the allograft in the comment section).
Clinically suspected rejection, not biopsy proven
In case of a clinically suspected rejection, that is not biopsy proven, enter the date of the suspected rejection in the date field of the Post-Transplant biopsy (even if the name is missleading). In ‘Type of biopsy’ and ‘Biopsy ID’ chose ‘missing’. Set the whole Banff score on ‘missing’ by selecting the ‘Mark all as missing’ button.
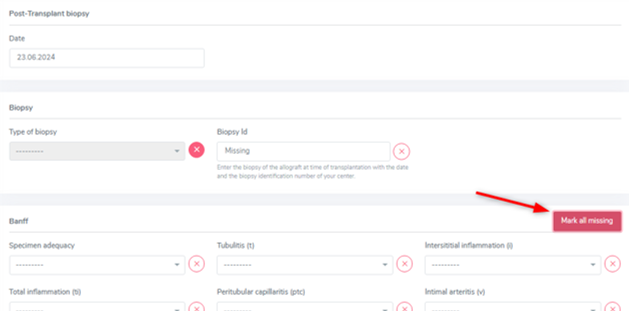
This will hide the Banff section.
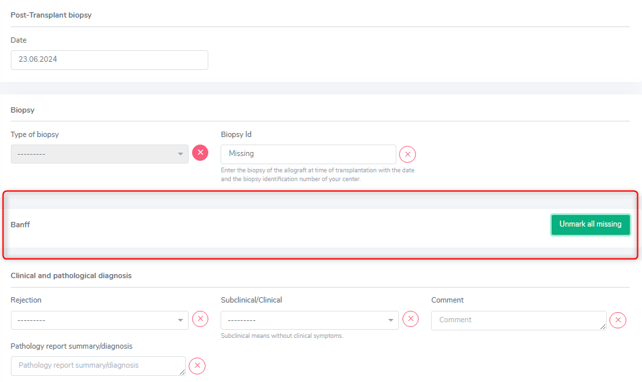
In the ‘Clinical and pathological diagnosis’ select ‘Clinically suspected, not biopsy proven’ in the Rejection section, choose between subclinical and clinical and set the ‘Pathology report summary/diagnosis’ to ‘missing’. Lastly enter all the applied treatment in the ‘Treatment’ section and save the whole section.
6.1.3. Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications, diseases and a possible loss of the organ.
Complication
In the complication section we collect major complications of the kidney allograft with the respective date of diagnosis. If the exact date is unknown, you can leave a comment in the comment section. The following complications are collected:
Biopsy-related complication
Hemorragic complication
Intraabdominal infection
Lymphocele
Obstruction
Renal artery stenosis/Kincking
Renal artery thrombosis
Renal vein thrombosis
Surgical site-infection and
Urine leak
Other
We also specify if the complication required a surgical intervention (select ‘Yes’ or ‘No’ accordingly or ‘Missing’ if you habe no information about the performance of a surgical intervention).
Do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be eintered in the stop form with the immediate and underlying cause of death.
Allograft Disease
If a biopsy or a medical report lists one of the following diagnosis, please enter them as ‘allograft disease’:
Acue tubular necrosis (ATN)
Chronic lesions, not specified
CNI nephrotoxicity
De novo glomerulonephritis/Vasculitis
Diabetic nephropathy
Graft pyelonephritis
Hemolytic uremic syndrome/ Thrombotic microangiopathy
PyVAN
Recurrence of initial disease or
Other (specifying a major disease of the allograft in the comment section).
In case the diagnosis is biopsy proven, please select ‘Yes’ and choose the Biopsy ID from the drop-down list that is shown.
Graftloss
A graft loss is the loss of function of the kidney. It implies the end of data collection of this specific orgen but only of the other, patientspecific data, PSQ and possible sample, if no other organ is actively followed in the system!
To enter a graft loss in the organ container, first set the toggle “graft loss”/ “End of transplant episode” in the kidney FUP to yes. Only after that, you will be able to access the ‘graftloss’ section in the kidney container.

If the kidney lost its function, enter the date of gradft loss (start of dialysis) and the cause of graft loss, selecting from:
Acute tubular necrosis (ATN)
Biopsy-related complication
Chronic allograft nephropathy(CAN)
CNI nephrotoxicity
Diabetic nephropathy
Graft pyelonephritis
Immunological
Intraabdominal infection
Obstruction
Primary non-function
PyVAN
Recurrence of initial disease
Renal artery stenosis/Kincking
Renal artery thrombosis
Renal vein thrombosis
Surgical site-infection
Thrombotic microangiopathy
Cause unknown
Other causes
In case of a re-transplantation the graft loss with its underlying disease will be shown per default as cause leading to (re-) TX.
6.2. Heart
In the heart container there are three sections:
Underlying disease (leading to transplantation)
Biopsy & Rejection and
Allograft morbidities.
6.2.1. Underlying disease
In this section, we select and confirm the condition leading to transplantation. To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other category. For example ‘HFpEF’ can be entered or as ‘Condition Leading to Tpx’ or as ‘Cardio-pulmonary’. It will appear in both sections, regardless of where it has been entered.
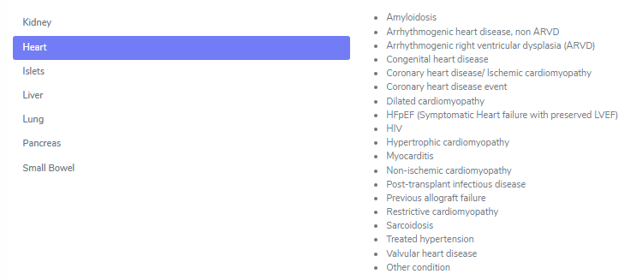
As conditions or diseases leading to transplantation in heart we select from the following:
All entered diagnosis will appear in the section ‘Underlying Disease’ and you must confirm the condition leading to transplantation.

The following cathegories only need confirmation:
Amyloidosis
Arrhythmogenic heart disease, non ARVD
Arrhythmogenic right ventricular dysplasia (ARVD)
Congenital heart disease
Coronary heart diseae/Ischemic cardiomyopathy
Coronary heart disease
Hypertrophic cardiomyopathy
Myocarditis
Non-ischemic cardiomyopathy
Restrictive cardiomyopathy
Sarcoidosis
Treated hypertension
Cardiac valvular disease and
Other conditions
The dilated cardiomyopathy asks you to choose the type of dilated cardiomyopathy from:
Genetic
Idiopathic
Myocarditis
Toxic and
Other.
HFpEF asks you to choose the type of HFpEF from:
Amyloidosis and
Restrictive cardiomyopathy.
6.2.2. Biopsy & Rejection
In this section we enter biopsies and rejections. We distinguish between ‘Time zero and reperfuion biopsies’ and ‘Post-transplant biopsies’.
Time zero and reperfusion biopsy
In the case of a time zero or reperfusion biopsy we enter the:
Date of the biopsy
Biopsy ID
Type of biopsy • Pre-implantation (allograft) • At reperfusion or • Native organ
If the biopsy lists one of the following diagnosis, please enter them in the ‘Allograft morbidities‘ section as ‘allograft disease’:
Recurrence of initial cardiac disease
Infection other than surgical site
CNI-induced toxicity or
Other (specifying a major disease of the allograft in the comment section).
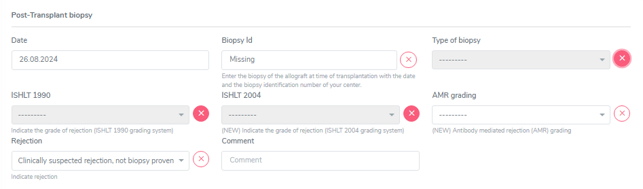
Post-Transplant biopsy and rejection
In the case of a biopsy performed after transplantation, we enter the date of the:
Biopsy
Biopsy ID
Type of biopsy:
Diagnostic biopsy
Protocol biopsy
Biopsy of associated organ in combined tpx or
other
ISHLT 1990 and/or ISHLT 2004 score
AMR grading
Rejection.
In the ‘Rejection’ part, we choose between:
Yes, biopsy proven
Yes, clinically suspected or
No.
When you select a ‘Yes’-option in the rejection field, you can choose the regimen(s) to treat this rejection in the section that appears below. Select all that apply from the following list and do not forget to enter the treatment in the ‘Treatment’ section as drug prescription or non-pharmacological treatment:
No treatment of rejection
ATG
ATGAM
Campath
IG iv
Metyl-prednisone iv
OKT3
Photopheresis
Plasmapheresis/PE
Prednisone po
Rituximab
Thymoglobulin
Other (Specifying the treatment in the comment field)
If the biopsy lists one of the following diagnosis, please enter them in the ‘Allograft morbidities‘ section as ‘allograft disease’:
Recurrence of initial cardiac disease
Infection other than surgical site
CNI-induced toxicity or
Other (specifying a major disease of the allograft in the comment section).
Clinically suspected rejection, not biopsy proven
In case of a clinically suspected rejection, that is not biopsy proven, enter the date of the suspected rejection in the date field of the Post-Transplant biopsy (even if the name is missleading). In ‘Biopsy ID’ and ‘Type of biopsy’ chose ‘missing’ and do the same for ‘ISHLT 1990’, ‘ISHLT 2004’ and ‘AMR grading’. In ‘Rejection select ‘Clinically suspected, not biopsy proven’ and then enter all the applied treatment in the ‘Treatment’ section that pops up. Lately save the whole section.
6.2.3.Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications, diseases, interventions and a possible loss of the organ.
Complication
In the complication section, we collect major complications of the heart allograft with the respective date of diagnosis. If the exact date is unknown, you can leave a comment in the comment section. The following complications are collected:
Air embolism
Biopsy-related complication
CVI, Chronic venous insufficiency
Diaphragma paralysis
Hemorrhagic complication
Lymphocele
Surgical site-infection and
Other.
The biopsy-related complication implies the question if there was biopsy-related tricuspid regurgitation complication yes or no.
Warning
Do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be eintered in the stop form with the immediate and underlying cause of death.
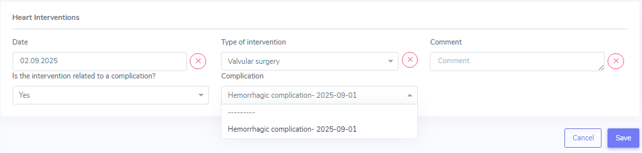
Interventions
In the cardiac interventions we collect the date of the intervention and the type of intervantion. If the exact date is unknown, you can leave a comment in the comment section. The following interventions are collected:
Valvular surgery
Bypass surgery
Percutaneous coronary intervention
Device implantation and
Other
Moreover you have to indicate if the intervention is related to a complication (yes or no) and if yes, select the complication that lead to the intervention from the shown drop-down list.
Graft loss
A graft loss is the loss of function of the heart. It implies the end of data collection of this specific organ and a possible re-transplantation.
To enter a graft loss in the organ container, first set the toggle “graft loss” in the heart FUP to yes. Only after that, you will be able to access the ‘graftloss’ section in the kidney container.

If the heart lost its function, enter the date of graft loss and the cause of graft loss, selecting from:
Arryhtmia
Immunological
Primary graft dysfunction
Recurrence of initial cardiac disease
Right heart failure
Transplant vasculopathy (CAV) with acute ischemia
Transplant vasculopathy (CAV) with chronic ischemia
Cause unknown or
Other causes.
In case of a re-transplantation the graft loss with its underlying disease will be shown per default as cause leading to (re-) TX.
6.3. Islets
In the islets container there are three sections:
Underlying disease (leading to transplantation)
Reperfusion
Biopsy & Rejection and
Allograft morbidities
6.3.1. Underlying disease
In this section, we select and confirm the condition leading to transplantation. To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other cathegory. For example ‘Cystic fibrosis (CF)’ can be entered or as ‘Condition Leading to Tpx’ or as ‘metabolic’. It will appear in both sections, regardless of where it has been entered.
As conditions or diseases leading to transplantation in islets we select from the following:

Diabetes type 1 is not on the list, but the main condition leding to islets transplantation. It can be chosen in ‘Metabolic’ or ‘Condition leading to Tpx’ never the less.
In Islets all the diagnosis only need a confirmation without the adding of further information.
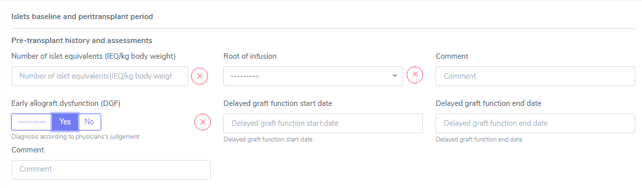
6.3.2. Reperfusion
A reperfusions differs from a re-transplantation of islets. In Zurich, the cutoff for differentiating them is the value of the C-peptide. We create a re-transplantation with a C-peptide <100pmol/l and a reperfusion if the C-peptide is >100pmol/l. The final decision of definition is a matter for the doctors. Please ask your ohn physician if the transplanted islets are considered a reperfusion or a re-transplantation. In case of a re-transplantation, please do not forget to enter a graftloss prior to the re-transplantation. Also in Zurich, per definition the cause of graft loss is always to be entered as ‘Cause of graft loss: other «either rejection or recurrence of autoimmunity».
After entering all the relevant information, a baseline is created and needs to be completed as any other baseline. For the relevant information go to the respective chapters in this manual.

The section ‘Reperfusion BL’ corresponds to the ‘Islets BL’.
Multiple Reperfusions can be added by choosing the ‘+’ on the right side. Be careful to enter the reperfusion in the corresponding islets transplantation.
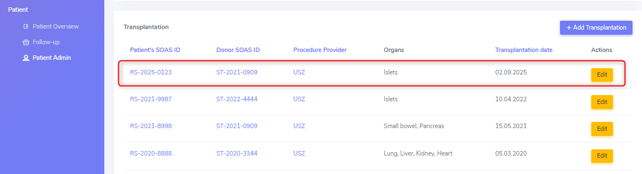
The reperfusion, even if technically corresponding to a transplantation, will not be shown in the patient overview. It is however, visible in the patient Admin under ‘Transplantation’ and in the Islets container in ‘Reperfusion’.
Warning
Only collect Samples prior to re-perfusion (i.e. “0” Sampling ) (SOP 03.09.2015)
6.3.3. Rejection
In this section we enter rejections in islet transplantations. Other than in solid organs, there is no option to perform biopsies on islets. Therefore rejections are collected based on clinical symptoms or suspected rejection based on a biopsy result of a co-transplanted organ, usually kidney.
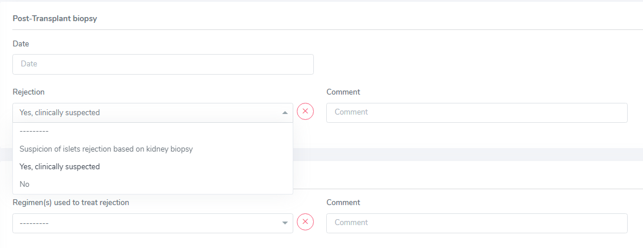
The section is missleadingly called ‘Post-transplant biopsy’, but as explained, no biopsy has to be entered.
We only collect the date of diagnosis of rejection, the type of rejection (Selecting from ‘Yes, clinically suspected’ or ‘Suspicion of islets rejection based on kidney biopsy’) and all the regimen(s) used to treat the rejection in the ‘Treatment’ section.
Clinically suspected rejection, not biopsy proven
In case of a clinically suspected rejection, that is not biopsy proven, enter the date of the suspected rejection in the date field of the Post-Transplant biopsy (even if the name is missleading). As ‘Rejection’ type select ‘Yes, clinically suspected’ and all the regimen(s) used to treat the rejection in the ‘Treatment’ section.
6.3.4. Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications and a possible loss of the organ.
Complication
Possible islets-transplant related complications are:
Bleeding
Portal vein thrombosis and
Other.
Do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be entered in the stop form with the immediate and underlying cause of death. In islets we do not collect any tx-related interventions. Therefore no link has to be created between a complication and an intervention.
Graft loss
A graft loss is the loss of function of the islets. It implies the end of data collection of this specific organ but only of the other, patient specific data, PSQ and possible sample, if no other organ is actively followed in the system!
To enter a graft loss in the organ container, first set the toggle “graft loss” in the islets FUP to yes. Only after that, you will be able to access the ‘graftloss’ section in the islets container.

If the islets lost their function, enter the date of graft loss and select if it was a primary non-function or not. No case of graft loss has to be selected.
In case of a re-transplantation the graft loss with its underlying disease will be shown per default as cause leading to (re-) TX.
6.4. Liver
In the liver container there are three sections:
Underlying disease (leading to transplantation)
Biopsy & Rejection and
Allograft morbidities.
As the fields might require the indication of a biopsy or related complication, it is best to enter the ‘biopsy & rejection’ as well as the requested information of the ‘allograft morbidities’ section following the order they appear in 3LC.
6.4.1. Underlying disease
In this section, we select and confirm the condition leading to transplantation. To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other cathegory.
For example, ‘Diabetes mellitus type 1’ can be entered or as ‘Condition Leading to Tpx’ or as ‘Metabolic’. It will appear in both sections, regardless of where it has been entered.
As conditions or diseases leading to transplantation in liver we select from the following:

All entered diagnosis will appear in the section ‘Underlying Disease’ and you must confirm the condition leading to transplantation.

All diagnosis that are not explicitly mentioned below and apart of previous allograft failure, only request a biopsy and the date of this biopsy if the condition was histologically confirmed.
Warning
Be careful when entering the Biopsy ID that confirmed the disease and not just a biopsy of the native organ. In case of two or more conditions leading to the same transplantation, the biopsies showing the diseases could be different one from another (e.g. one showing the hepatitis and a later one showing the HCC). Use the first biopsy that confirmed the disease.

Hepatitis B and C
In case of a hepatitis B or C leading to transplantation, you are asked for the course of the liver disease –‘fulminant hepatitis’ or ‘chonic hepatitis’ – as well as if the disease has been confirmed by biopsy. If so, enter the date and the ID of the diagnostic biopsy.
HCC and other liver tumors as cause leading to TPX
This section covers the following diagnosis leading to transplantation:
Epitheloid hemangioendothelioma
Hepatocellular carcinoma (HCC)
Neuroendocrine tumor
Cholangiocarcinoma
Other liver cancer
In liver patients in case of a HCC or an other liver tumor leading to transplantation, when confirming it, tumor specific information for different points in time is requested.
There is a general section for tumorspecific information as well as a tumor therapy section in the upper part, followed by tumor staging at different points in time. The timepoints of specific data collection before transplantation are:
at diagnosis
at listing evaluation and
pretransplant.
The same information is requested for these different timepoints. If at one of the given stages no staging has been done, set the whole section to ‘Missing’ with the ‘Mark all Missing’ butten on the right.

Liver Underlying Disease – Tumor Specification
In this section, please enter a possible explantation biopsy by selecting ‘yes’ and specifying the according biopsy number.
Note
The gray fields show historic values (values that were entered in the old system) and no entries can be made here.

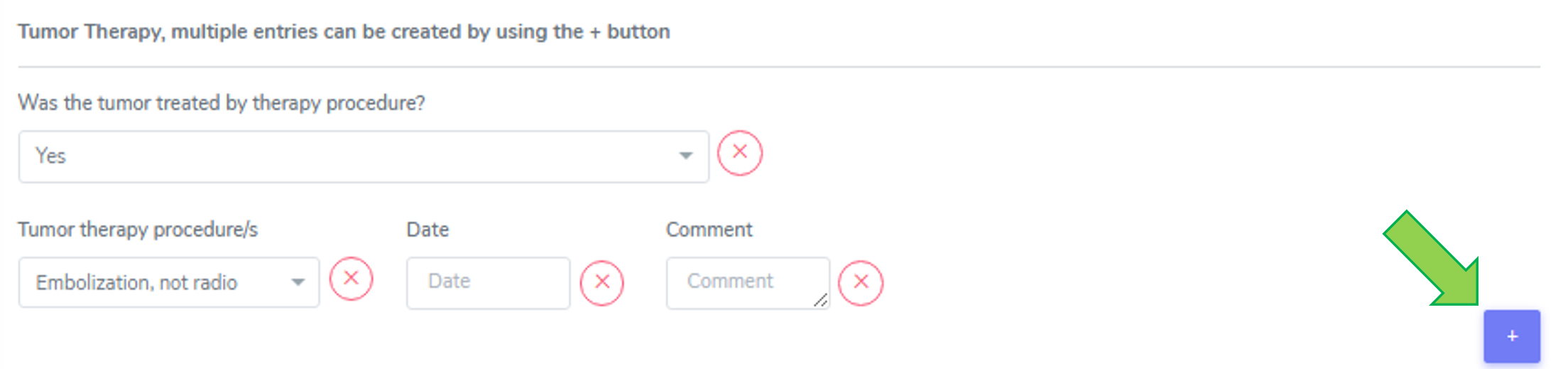
Tumor Therapy
If the tumor was treated, select ‘yes’ and enter the tumor therapy preocedure(s) and the date it was performed.
Enter all treatments, even if one was done more than once. We enter all of the following therapies:
Embolization, not radio
Microwave ablation (MWA)
Radiofrequency ablation (RFA and RFTA/ Radiofrequency thermoablation)
Selective internal radiation therapy (SIRT)
Systemic therapy (like Chemotherapy or immuneotherapy) and
Trans-arterial chemoembolization (TACE), includes TAE!.
Multiple entries can be created by using the (+) button (see green arrow).
Liver Underlying Disease – Tumor Specification
In this section, please enter a possible explantation biopsy by selecting ‘yes’ and specifying the according biopsy number. The gray fields show historic values (values that were entered in the old system) and no entries can be made here.

Tumor Therapy
If the tumor was treated, please select ‘yes’ and enter the tumor therapy preocedure(s) and the date it was performed.
Please enter all treatments, even if one was done more than once. We enter all of the following therapies:
Embolization, not radio
Microwave ablation (MWA)
Radiofrequency ablation (RFA and RFTA/ Radiofrequency thermoablation)
Selective internal radiation therapy (SIRT)
Systemic therapy (like Chemotherapy or immuneotherapy) and
Trans-arterial chemoembolization (TACE)
Warning
The therapy trans-arterial chemoembolization (TACE) also includes TAE!
Multiple entries can be created by using the (+) button.
Tumor Staging (at Diagnosis, at Listing Evaluation and Pretransplant)
Every staging timepoint (at Diagnosis, at Listing Evaluation and Pretransplant) requires the same information: If the tumor was confirmed by imaging diagnosis ‘yes’, ‘no’ or ‘missing’.
If yes, enter the date of the imaging diagnosis and select the method used. The imaging methods are listed from the most sensitive/accurate to the least sensitive/accurate method:
MRI and CT
MRI
Conventional CT
PET CT or
Ultrasound
Use the most sensitive used imaging method from the list and complete the missing information.
For all cases, please enter the date of the imaging, the number of active leasions found in the imaging as well as the size (in mm) of the largest tumor lesion. Further, indicate if the tumor staging at this timepoint timepoint (at Diagnosis, at Listing Evaluation and Pretransplant) is inside or outside the Milan criteria.
Tip
Definition of Milan criteria (Tumor size and number): either a single tumor with a diameter of ≤ 5 cm or no more than three tumors, with each tumor measuring ≤ 3 cm in diameter.
Please indicate if in the biopsy or per imaging diagnosis macrovascular invasion was detected (‘yes’, ‘no’, or ‘missing’).
Moreover we enter the Biopsy ID of the biopsy taken at this timepoint (at Diagnosis, at Listing Evaluation and Pretransplant) and the according histopathology biopsy ID. If there is no staging at a certain timepoint, choose the red ‘missing’ button to set all the values to missing.

Definitions regarding the timepoint of the tumor staging:
Tumor staging at Diagnosis: last staging before diagnosis
Tumor Staging at Listing Evaluation last staging (closest) before listing
Tumor Staging Pretransplant last staging before transplantation
6.4.2. Biopsy & Rejection
In this section, we enter biopsies and rejections. We distinguish between ‘Time zero and reperfusion biopsies’ and ‘Post-transplant biopsies’.

Peri-transplant biopsy
In the case of a time zero or reperfusion biopsy we enter the date of the biopsy, the Biopsy ID, the type of biopsy:
Pre-implantation (allograft)
At reperfusion or
Explantation biopsy
as well as:
the amount of macrosteatosis (Use 0 to indicate absence of steatosis. Use 100% to indicate above some limit e.g. > 80% or select ‘Missing’ if there is no clear indication of macrosteatosis)
the presence of microsteatosis (‘Present’, ‘Absent’ or ‘Missing’) and
the levelof fibrosis (‘Absence of fibrosis’, ‘F1’, ‘F2’, ‘F3, ‘F4’ or ‘Missing’)
Post-Transplant biopsy and rejection
In the case of a biopsy performed after transplantation, we enter the date of the biopsy, the Biopsy ID, the type of biopsy:
Diagnostic biopsy
Protocol biopsy or
Other.
We collect the following infoormation of this biopsy:
The RAI score, where we select the RAI score of the biopsy.
the amount of macrosteatosis (Use 0 to indicate absence of steatosis. Use 100% to indicate above some limit e.g. > 80% or select ‘Missing’ if there is no clear indication of macrosteatosis.)
the presence of microsteatosis (‘Present’, ‘Absent’ or ‘Missing’)
the level of fibrosis (‘Absence of fibrosis’, ‘F1-F4’, or ‘Missing’)
the portal inflammation (Score 1-4 or ‘Missing’)
the bile duct inflammation damage (Score 1-3 or ‘Missing’) and
the venous endothelial inflammation (Score 1-3 or ‘Missing’).
In case a value is not done or can not be evaluated, please choose ‘missing’. You also have the option to choose ‘All missing’ if there no biopsy was done and only a possible rejection was treated.
If there are multiple scores for fibrosis (e.g. F2-F3) or steatosis, then enter the highest value.
In the ‘Rejection’ part, we enter the rejection (‘Yes, biopsy proven’, ‘Yes, clinically suspected’ or ‘No’.). When you select a ‘Yes’-option in the rejection field, you can choose the regimen(s) to treat this rejection in the ‘Treatment’ section that appears below.
Select all that apply from the following list and do not forget to enter the treatment in the ‘Treatment’ section as drug prescription or non-pharmacological treatment:
No treatment of rejection
ATG
ATGAM
Campath
IG iv
Metyl-prednisone iv
OKT3
Photopheresis
Plasmapheresis/PE
Prednisone po
Rituximab
Thymoglobulin
Other (Specifying the treatment in the comment field)
Clinically suspected rejection
In case of a clinically suspected rejection, that is not biopsy proven, enter the date of the suspected rejection in the date field of the Post-Transplant biopsy (even if the name is missleading) and set the whole biopsy section on ‘missing’ (‘Mark all missing’).

In the rejection section enter ‘Yes, clinically suspected’ and in the treatment section select all the regimens used to treat that suspected rejection.
If there was a suspected rejection that was not treated, select ‘No treatment of rejection’.
6.4.3. Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications, interventions, allograft diseases, and a possible loss of the organ.
Complications
In the complication section, we collect major complications of the liver allograft with the respective date of diagnosis. If the exact date is unknown, you can leave a comment in the comment section.
The following complications are collected:
Abdominal abscess
Acute hepatic artery thrombosis (HAT)
Anastomotic biliary stricture (AS)
Arterial stenosis
Biliary leak
Biopsy-related complication
Bleeding
Bowel perforation
Chronic hepatic artery thrombosis (HAT)
Portal vein thrombosis
Surgical site-infection
cava thrombosis/ stenosis
Other and
Non-anastomotic biliary stricture (NAS).
You also need to indicate the Dindo-Clavien grading of the complication (I-V or missing).
The therapy used to correct a specific complication is the basis of this classification in order to rank a complication in an objective and reproducible manner.
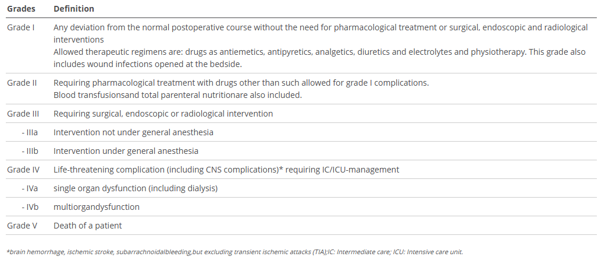
We only collect the stages I-V without sub-groups.
Do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be entered in the stop form with the immediate and underlying cause of death.
Interventions
We collect the following type of interventions:
Endoscopic intervention - as “endoscopic intervention” we consider things like gastroscopies, ERCP and interventions performed during an ERCP.
Pharmacological intervention - as “pharmacological intervention” we consider treatments like a benzafibrat given to treat biliary stenosis.
Radiological intervention and
Surgical intervention - as “surgical intervention” we consider all interventions that were performed in the OR under general anaesthesia and in Dindo-Clavien grading are grade IIIb (classified as grade III in 3LC).
Please indicate if the intervention is related to a complication. If so, select the according complication from the dropdown list. To do so, the complication must first be entered in the complication section.
Allograft disease
In the allograft disease section we enter three categories of diseases:
De novo disease
Recurrence of initial disease and
Cirrhosis.
All must be completed by a (diagnosis) date. This date does not have a date-accuracy field. Therefore, please use the comment field if you need to make an indication of an approximation regarding the indicated date.
The first two of these cathegories need further specification:
The ‘De novo disease’ must be selected from:
Alcoholic liver disease
Autoimmune hepatitis
Chronic rejection
Hepatocellular carcinoma (HCC)
NASH or
Other.
The ‘recurrence of initial disease’ can be selected from the dropdown list that appears and which includes the diagnosis indicated in the cathegory ‘Condition leading to Tpx’ in the ‘Patient Diagnosis List’ container.
In all cases, please indicate if the allograft disease is biopsy proven. If so, select the according biopsy from the dropdown list. To do so, the biopsy must first be entered in the biopsy and rejection section.
Graftloss
A graftloss is the loss of function of the liver. It implies the end of data collection of this specific organ but only of the other, patient specific data and possible sample, if no new organ is transplanted.
To enter a graftloss in the organ container, first set the toggle “Graftloss” in the liver FUP to “yes”. Only after that, you will be able to access the ‘graftloss’ section in the liver container.

When the liver loses its function, enter the date of graftloss and the cause of graft loss, selecting from:
De novo causes
Recurrence of initial disease
Cirrhosis
Cause unknown or
Primary non-function.
When selecting ‘De novo causes’, meaning a new onset diagnosis after transplantation, not present in the native or in a previously transplanted liver, please chose the cause from the following list:
Acute rejection (Immunological)
Anastomotic biliary stricture (AS)
Alcoholic liver disease
Arterial thrombosis
Autoimmune hepatitis
Chronic rejection
Fulminant hepatitis
Hepatocellular carcinoma (HCC)
NASH
Non-anastomotic biliary stricture (NAS) or
Other.
When selecting ‘Recurrence of initial disease’ select the according disease from the dropdown list.
In case of a ‘Primary non-function’, select the cause of the PNF from the following list:
Hyperacute rejection
Arterial thrombosis
Portal vein thrombosis
Graft quality
Cause unknown or
Other causes.
In case of a re-transplantation the graftloss with its underlying disease will be shown per default as cause leading to transplantation.
6.5. Lung
In the lung container, there are three sections:
Underlying disease (leading to transplantation)
Biopsy & Rejection and
Allograft morbidities.
6.5.1. Underlying disease
In this section we select and confirm the condition leading to transplantation. To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other cathegory. For example ‘Cystic fibrosis’ can be entered or as ‘Condition Leading to Tpx’ or as ‘Metabolic’. It will appear in both sections, regardless of where it has been entered.
As conditions or diseases leading to transplantation in liver we select from the following:
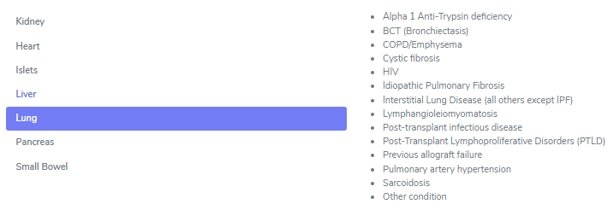
All entered diagnosis will appear in the section ‘Underlying Disease’ and you must confirm the condition leading to transplantation, as shown below.

All diagnosis (except ‘Cystic Fibrosis’) only request a confirmation of the condition leading to transplantation.
Idiopatic Pulmonary fibrosis
Cystic Fibrosis
When selecting Cystic Fibrosis (CF) as condition leading to TPX, you need to select if there were (or are) any airway pathogens present in the timeframe from 1 year before transplantation until transplantation.
If yes, choose all that apply from the following selection:
Mycobacterium other than tuberculosis, MOTT
MRPSA
Achromobacter xylosoxidans
Candida albicans
Candida non albicans
Aspergillus fumigatus
Burkholderia cenocepacia
Burkholderia other
MSSA
MRSA
Pseudomonas aeruginosa
Stenotrophomonas and/or
Other (please specify in the comments).
6.5.2. Biopsy & Rejection
In this section we enter biopsies and rejections. We distinguish between ‘Peri-transplant biopsies’ and ‘Post-transplant biopsies’.

Peri-transplant biopsy
In the case of a time zero or reperfusion biopsy, we enter:
the date of the biopsy,
the Biopsy ID
the type of biopsy:
Pre-implantation (allograft)
At reperfusion or
Explantation biopsy.
Post-Transplant biopsy and rejection
In the case of a biopsy performed after transplantation, we enter:
the date of the biopsy
the biopsy procedure:
Surgical biopsy
Transbronchial biopsy or
Cryobiopsy
the type of biopsy:
Diagnostic biopsy
Protocol biopsy or
Other and the the Biopsy ID.
In case of a Transbronchial biopsy or a Cryobiopsy, you have to select if the performed bronchoscopy was an:
Indication or a
Surveillance bronchoscopy.
Note
In both cases it is set to ‘indication’ per default. You can change it to ‘surveillance’ manually.
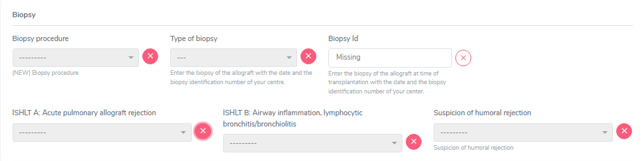
In the ISHLT section select the scores indicated in the pathology report:
ISHLT A: Acute pulmonary allograft rejection (1-4 or X)
ISHLT B: Airway inflammation, lymphocytic bronchitis/bronchiolitis (0, 1R, 2R or X) and
Suspicion of humoral rejection (Excluded, Possible, Probable, Definite).
Tip
If there are multiple scores for ISHLT A, B an/or suspected humoral rejection, (e.g. ISHLT A 1-2) then enter the highest indicated value.
In the ‘Rejection’ part, we enter if the rejection is biopsy proven, clinically suspected or if there is no rejection. If necessary, a comment.
When you select a ‘Yes’-option in the rejection field, you can choose the regimen(s) to treat this rejection in the ‘Treatment’ section that appears below. Select all that apply from the following list and do not forget to enter the treatment in the ‘Treatment’ section as drug prescription or non-pharmacological treatment:
No treatment of rejection
ATG
ATGAM
Campath
IG iv
Metyl-prednisone iv
OKT3
Photopheresis
Plasmapheresis/PE
Prednisone po
Rituximab
Thymoglobulin
Other (Specifying the treatment in the comment field)
Clinically suspected rejection (not biopsy proven)
In case of a clinically suspected rejection, which is not biopsy proven, enter the date of the suspected rejection in the date field of the Post-Transplant biopsy (even if the name is missleading).
In ‘Biopsy procedure’, ‘Type of biopsy’ and’ Biopsy ID’ as well as in ‘ISHLT A’, ‘ISHLT B’ and ‘suspicion of humoral rejection’ chose ‘missing’.
In the ‘Rejection’ section, select ‘Yes, clinically suspected’, then enter all the applied treatments in the ‘Treatment’ section and save the form.
6.5.3. Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications leading to a re-operation, allograft diseases, and a possible end of lung tpx episode (graft loss).
Complication leading to re-operation
Select from the following transplant-related complications leading to re-operation:
Anastomosis, vascular
Anastomosis, airway
Chest wall complication
Extra-thoracic conditions
Haemorrhage
Pleural space complication or
Other.
Complications not leading to a re-operation are not collected. Therefore do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be entered in the stop form with the immediate and underlying cause of death.
Allograft disease
In this section, we enter graft diseases with the date of diagnosis selecting from:
CLAD (chronic lung allograft dysfunction)
Histologically proven recurrence of initial lung disease
Primary pulmonary tumor or pulmonary PTLD
Pulmonary (arterial) hypertension
Pulmonary infection or
Other.
Note
Usually the form of CLAD (RAS or BOS) are no longer specified. But if you do have an information about it, please enter it in the comment field.
Moreover, indicate if the graft disease is biopsy proven (Yes/No) and if so, select the Biopsy ID from the dropdown. To do so, the biopsy must first be entered in the biopsy and rejection section.
End of transplant episode/Graft loss
The end of transplant episode is the section that in the other organs is called ‘graft loss’ and indicates the loss of organ function of the left lung, the right lung or the double lung. Please indicate which part(s) of the transplanted lung filed in ‘part of the lung that failed’.
To enter a graft loss in the organ container, first set the toggle “End of transplant episode” in the lung FUP to yes. Only after that, you will be able to access the ‘graftloss’ section in the kidney container.

If the lung has lost its function, enter the date of graft loss and the cause of graft loss, selecting from:
Acute humoral rejection
CLAD
Histologically proven recurrence of initial lung disease
Pulmonary infection
Technical / surgical complication (including biopsy related complications)
Cause unknown or
Other causes (such as aspiration, bronchial complications, pulmonary hypertension or tumor)
More than one option can be selected.
In case of a re-transplantation the graft loss with its underlying disease will be shown per default as cause leading to (re-) TX.
6.6. Pancreas
In the pancreas container, there are three sections:
Underlying disease (leading to transplantation)
Biopsy & Rejection and
Allograft morbidities.
6.6.1. Underlying disease
In this section we select and confirm the condition leading to transplantation. To do so, we first need to enter this condition or disease in the ‘Patient Diagnosis List’ as ‘Condition Leading to Tpx’ or in an other category.
For example, ‘Diabetes mellitus type 1’ can be entered or as ‘Condition Leading to Tpx’ or as ‘Metabolic’. It will appear in both sections, regardless of where it has been entered.
As conditions or diseases leading to transplantation in pancreas we select from the following:
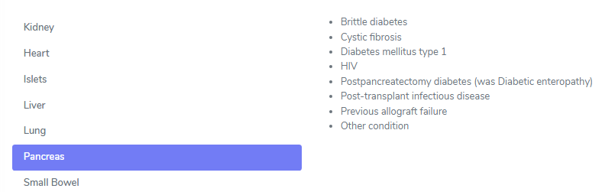
All entered diagnosis will appear in the section ‘Underlying Disease’ and you must confirm the condition leading to transplantation. No further information is requested when confirming the diagnosis leading to transplantation.
6.6.2. Biopsy & Rejection
In this section, we enter biopsies and rejections. In pancreas we only collect ‘Post-transplant biopsies’.

Post-Transplant biopsy and rejection
In the case of a Post-Transplant biopsy and rejection, we enter the date of the biopsy, the Biopsy ID, the type of biopsy.
The types of biopsy can be:
Diagnostic biopsy
Protocol biopsy
Biopsy of associated organ in combined tpx or
Other.
The type ‘Biopsy of associated organ in combined tpx’ refers i.e. to a kidney biopsy in an SPK transplantation.
Further, we select if there was a (suspected) rejection or not and we can choose between:
Yes, biopsy proven
Yes, clinically suspected
Suspicion of pancreas rejection based on kidney biopsy or
No.
In the ‘Clinical and pathological diagnosis’ part, we enter:
Rejection (Yes, biopsy proven; Yes, clinically suspected; No)
If the patient showed the presence or absence of clinical symptoms (clinical/subclinical)
The Pathology report summary/diagnosis (copy and paste this part from the biopsy report in whatever language the text is) and
If necessary, a comment.
In case of a (suspected) rejection, please choose the regimen(s) used to treat this rejection in the section that appears below:
No treatment of rejection
ATG
ATGAM
Campath
IG iv
Metyl-prednisone iv
OKT3
Photopheresis
Plasmapheresis/PE
Prednisone po
Rituximab
Thymoglobulin
Other (Specifying the treatment in the comment field)
Select all that apply from the list and do not forget to enter the treatment in the ‘Treatment’ section as drug prescription or non-pharmacological treatment:
In the ‘Rejection’ drop-down select ‘Yes, Clinically suspected’ and enter all the applied treatments in the ‘Treatment’ section. Then save the whole section.
6.6.3. Allograft morbidities
Although called ‘allograft morbidities’, this section collects complications, interventions and a possible loss of the organ.
Complication
In the complication section, we collect major complications of the pancreas allograft with the respective date of diagnosis. If the exact date is unknown, you can leave a comment in the comment section. The following transplant-related complications are collected:
Abdominal abscess
Arterial thrombosis
Biopsy-related complication
Bleeding
Bowel perforation
Pancreatitis
Peritonitis
Portal vein thrombosis
Surgical site-infection
Other
Note
Do not enter ‘death’ as a complication itself. You might collect complications leading to death, but the death itself has to be entered in the stop form with the immediate and underlying cause of death.
Interventions
We collect the following interventions:
Thrombectomy
Hemostasis
Drainage
Arterial reconstruction
Pancreatectomy
Abdominal wash out
Bland laparotomy
Other
Please indicate if the intervention is related to a complication. If so, select the complication from the dropdown list. To do so, the complication must be first entered in the complication section.
Graftloss
A graftloss is the loss of the whole function of the pancreas. It implies the end of data collection of this specific organ but only of the other, patientspecific data, PSQ and possible sample, if no other organ is actively followed in the system!
Note
A new onset insulin requirement after pancreas transplantation does not automatically correspond to an organ loss. The pancreas might only have a partial function. In the case of insulin requirement after transplantation, please ask the physician if the organ has lost its function completely before entering a graft loss. Do not forget to enter the start of insulin application in the treatment section.
Tip
To enter a graft loss in the organ container, first set the toggle “graft loss” in the pancreas FUP to yes. Only after that, you will be able to access the ‘graftloss’ section in the pancreas container (see red arrow in the figure below).

If the pancreas has lost its function, enter the date of graft loss and the cause of graft loss, selecting from:
Abdominal abscess
Acute rejection (Immunological)
Arterial thrombosis
Biopsy-related complication
Bleeding
Bowel perforation
Graft exhaustion/chronic rejection
Pancreatitis
Peritonitis
Portal vein thrombosis
Primary non-function
Recurrence of autoimmunity i.e. recurrence of type 1 diabetes
Surgical site-infection
Cause unknown
Other causes
In case of a re-transplantation the graft loss with its underlying disease will be shown per default as cause leading to (re-) TX.
6.7. Small Bowel
In construction